
Overview:
Obesity is a state of excess body fat accumulation, while the term “overweight” is defined as an excess of body weight for height. Normal body fat percentage in healthy men is 15-20%, in women 25-30%. The body mass index (BMI) is commonly used to define overweight and obesity as an indirect indicator of body fat.
BMI is calculated as weight/height2, with weight being in kilograms and height being in meters (otherwise, the equation is weight in pounds 0.703/height in inches2). Online BMI calculators are available.
Classification of obesity:
For adults:
Overweight is defined as a BMI greater than or equal to 25 to 29.9 kg/m2
- Obesity class I – BMI 30 to 34.9 kg/m 2
- Obesity class II – BMI 35 to 39.9 kg/m 2
- Obesity class III – BMI greater than or equal to 40 kg/m 2 (also named severe, extreme, or massive obesity)
The borderline of BMI is adjusted for Asian and South Asian populations, with overweight being classified as 23-24.9 kg/m2, and obesity as 25 kg/m2 or greater.
For children under 5 years of age:
- overweight is weight-for-height greater than 2 standard deviations above WHO Child Growth Standards median; and
- obesity is weight-for-height greater than 3 standard deviations above the WHO Child Growth Standards median.
For children aged between 5–19 years:
- overweight is BMI-for-age greater than 1 standard deviation above the WHO Growth Reference median; and
- obesity is greater than 2 standard deviations above the WHO Growth Reference median.
Comorbidities associated with obesity:
Obesity is associated with more than 200 potential comorbidities that are contributed to severe morbidity and mortality in obese individuals.
The most common and well-documented complications of severe obesity are diabetes, hypertension and hyperlipidemia, heart failure, metabolic syndrome and ischemic stroke. Obesity also increases mortality from a number of cancers, mental health problems, and overall decreased quality of life.
Etiology:
The etiology of obesity is multifactorial: wider than simply an imbalance between calorie intake and energy expenditure. The genetic predisposition and metabolic factors play a substantial role. Also contributing factors, such as lifestyle, endocrine status, race, sex, age, ethnic and cultural factors had huge impact on developing overweight, obesity and it’s complications.
Epidemiology:
United States statistics:
More than 100 million US adults aged 20 years or older have obesity, including over 22 million with severe obesity. The prevalence of obesity among US adults rose steadily from 19.4% in 1997 to 31.4% for the period January-September 2017.
International statistics:
In 2022 2.5 billion individuals aged 18 years and older were overweight, including over 890 million adults who were living with obesity. This represents 43% of adults aged 18 years and over (43% of men and 44% of women) who were overweight, an increase from 1990, when 25% of adults aged 18 years and over were overweight. Overweight frequency varied by region, from 31% in the WHO South-East Asia Region and the African Region to 67% in the Region of the Americas.
The global prevalence of obesity increased more than twofold between 1990 and 2022.
Once predominantly being a problem in a high-income country, overweight is on the rise in low- and middle-income countries.
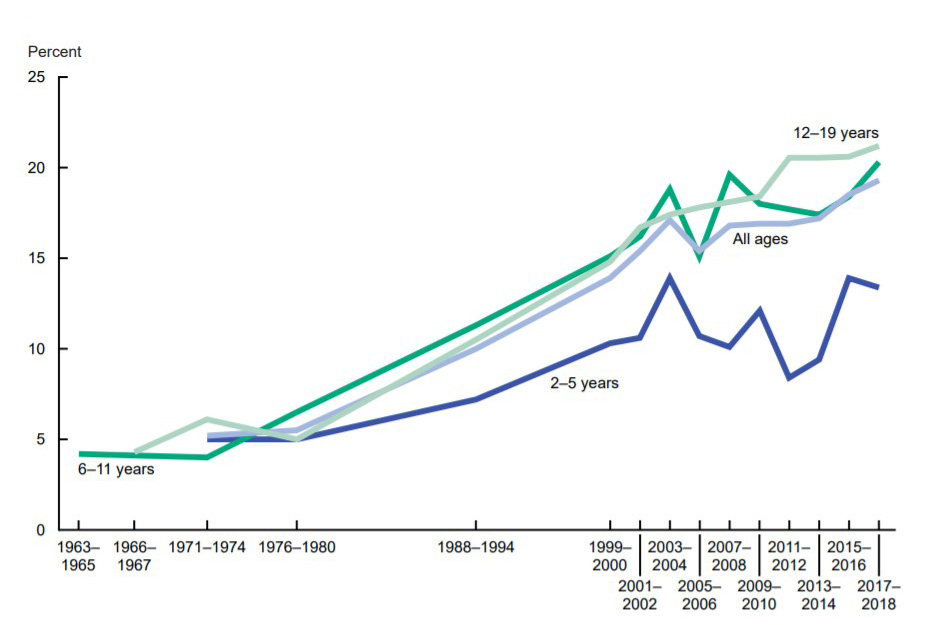
Image source: National Institute of Diabetes and Digestive and Kidney Diseases’s Overweight & Obesity Statistics
Prognosis:
Generally, obesity is supposed to increase the cardiovascular mortality rate fourfold and the cancer-related mortality rate twofold. People with BMI ≥40kg/m2 (severe obesity) have a 6- to 12-fold increase in the all-cause mortality rate. Obesity is undoubtedly the greatest preventable health-related cause of mortality after cigarette smoking. The risk of premature mortality is even greater in persons with obesity who smoke.
Prevention:
CDC’s ( U.S. Centers for Disease Control and Prevention) developed overweight and obesity prevention strategies based on promoting physical activity for people, statistical monitoring of overweight and obesity, developing and promoting diet and physical activity guidelines, making healthy food affordable for low-income families, creating communities with healthy lifestyles, referring people to the doctor in a timely manner, etc.
Treatment:
Treatment of obesity starts with extensive lifestyle management (i.e, diet, physical activity, behavior modification), which should include self-monitoring of caloric intake and expenditure, physical activity, goal setting, stimulus control, nonfood rewards and relapse prevention.
Pharmacologic therapy and bariatric surgery:
Several drugs are now available for the treatment of obesity. However, the benefits often diminished after discontinuation. Because of all medication’s intrinsic risks, pharmacologic therapy should be used only in patients in whom the benefit is more than with diet and exercise.
Surgery Well-performed bariatric surgery in properly selected patients managed by a multidisciplinary support team strongly improve the morbidities associated with severe obesity.
")





